
The new, more infectious B117 variant of COVID is a big deal, and it will significantly impact what the US will look like over the next few months.
Of note:
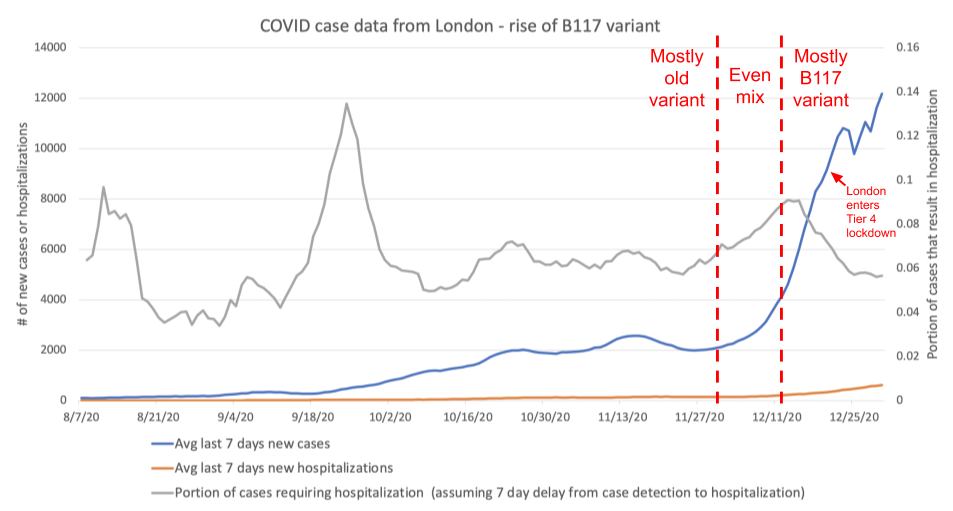
- The B117 variant is 50-70% more infectious. This may not seem like a lot, but it's likely the difference between being able to keep caseload under control while still having some nonessential activity vs a situation where caseload keeps going up uncontrollably unless you do something like the hard lockdown we had last March/April. We're seeing this in London right now; we'll know in the next few days if they manage to get the caseload to finally level off after enacting a stricter lockdown.
- The new variant appears to have similar hospitalization and mortality rates to the old one.
- There's a lot we don't know yet about how the greater infectiousness manifests, so there's a scary margin of uncertainty where we can't entirely trust the risk models that were developed last year. While tools like microCOVID can still serve as very rough guides, it's more precarious to find a safe middle ground that still allows for a lot of adventuring.
Unfortunately, this means my prior approach of "go have amazing outdoor adventures traveling all over the western US while wearing very good masks and staying physically distant or carefully crafting temporary travel pods via quarantines" isn't a reliable way of staying safe anymore. It's most likely still very safe to go out walking or hiking in a sparsely populated area while wearing a good mask, but it's hard to say what's OK beyond that.
- It took about 3 months for the B117 variant to go from being a tiny fraction of cases in the London area to being nearly all the cases in the London area. There's some unknown number of B117 cases in the US. We don't know if it's a tiny handful or several thousand because we don't do the same level of genetic variant testing like the UK does. The B117 variant will be dominant by sometime in March. We can slow B117 down and buy ourselves some time by being more careful now.
- As we talked about early last year, it's really bad if hospitals get overloaded. Mortality rates go way up because people can't get straightforward but lifesaving care.
- The vaccine is expected to work on the new variant, but so far US is completely bungling vaccine distribution, which ought to be the easiest part of the whole process. This isn't just because of Trump hollowing out federal institutions, it's decaying institutional expertise at basic logistics, planning, and decision-making that's manifesting at the state level as well. It's a sign that the US needs to radically increase its investment in government institutions at all levels, or at least outsource it to companies who know how to execute. This failure is a serious shame because scientists and engineers and project managers worked incredibly hard to get a fundamentally new kind of vaccine designed, tested, and produced at scale in a stunningly short amount of time. There's also significant delay because the distribution plan has a complex tiered system for maximally ethical distribution according to some metric, but complex plans are harder to execute, especially if you're totally unprepared. At this point, a handful of states have switched over to a first-come first-serve system for all high risk groups, and that will probably save more lives as it gets more vaccines in people's bodies faster. I'm sure future ethics students will be writing essays about the decisions made over the next few months.
- With the new variant almost guaranteed to take over in the next 3-5 months, we have very limited levers we can pull if we want to prevent another full lockdown. First, the government should be willing to throw near-infinite amounts of money at vaccine distribution and/or outsource it to a medical entity that knows how to execute at scale Vaccines are the only thing that can fully end the pandemic, and every day that they go unused is another day that society is shut down. Even though it will take most of the year to vaccinate everyone, every bit that we accelerate the timeline makes it easier to fight the disease at a societal level. Second, we should get everyone to upgrade their masks. Well-fitting N95s are far better than cloth masks, and ought to be the minimum acceptable standard for use in essential businesses and higher traffic areas. Both vaccines and masks are far cheaper than another hard lockdown. Separately, it's worth curtailing nonessential activities to buy us more time before B117 takes over, because it's going to be very painful to stop B117 once it's dominant.
More anecdotally, I've started hearing the first stories of people I know who are taking really good precautions but are still getting COVID. I don't know if this is due to the new variant or not, but it seems worth noting.
If you want to read more, the UK's technical briefing is fairly approachable: https://assets.publishing.service.gov.uk/.../Technical...
Also see:
https://www.theatlantic.com/.../virus-mutation.../617531/
And a technical paper with some impressively detailed modeling to reverse-engineer parameters of the new variant:
https://www.medrxiv.org/.../2020.12.24.20248822v1.full.pdf
UPDATE: We now have somewhat better prevalence data on B117 in the US. It's currently about 0.16%, and my friend Mike estimates it will be dominant around May: https://www.facebook.com/MikeCaptnKidd/posts/10217284743022297
Originally published on Facebook